urban teaching


urban teaching

(Note: This essay is still in draft form. A pdf file containing it is available here.)
This title can have more than one meaning; the one I intend is the one that isn't obvious. I'll explain.
What follows is an example of what can come out of multidisciplinary inquiry.
Lesson 1. My wife Ruth is a licensed mental health counselor; one of her specialties is working with people who have had trauma (both big-T and little-t) in their lives. This summer she took a one-week course taught by Bessel van der Kolk, MD, a well recognized trauma investigator and clinician [1]. The subject of the course was observable changes to the brains–and to the behaviors–of trauma victims. I spent the days in the library and was briefed from her notes at the end of each day.
Bottom line. Many victims of psychological trauma have major attention deficits as the result of their traumas. There can be a lot of overlap between the symptoms of ADHD and Post Traumatic Stress Disorder. [2] It is possible to confuse hypervigilance associated with PTSD with “hyperactivity.” If such hypervigilance is not noted a diagnosis of PTSD can fall through the cracks and show up simply as a learning disorder.
Some clinicians use the term of art not present to describe the cognitive state of some trauma victims. Every teaching day of my four years at Chelsea High School I looked into the faces of many people who were not present.
Lesson 2. Several therapists taking the course stayed in the same B&B where we were, and breakfast conversations were lively with shared experiences. One person suggested that I learn about the ACE study, and I spent that day researching it. What an eye-opener that was. “ACE” stands for “adverse childhood experiences.” The initial study examined the emotional histories of over 17,000 adult patients at Kaiser Permanente, and correlated these histories with adult morbidity. To quote from the first page of a 2002 paper [3] I strongly recommend to every reader:
“The ACE Study reveals a powerful relationship between our emotional experiences as children and our physical and mental health as adults, as well as the major causes of adult mortality in the United States. It documents the conversion of traumatic emotional experiences in childhood into organic disease later in life. How does this happen, this reverse alchemy, turning the gold of a newborn infant into the lead of a depressed, diseased adult? The Study makes it clear that time does not heal some of the adverse experiences we found so common in the childhoods of a large population of middle-aged, middle class Americans.”
The researchers defined a number from 0 to 8 called the “ACE Score.” This number counts the number of different categories of childhood abuse and household dysfunction (not the number of incidents) reported by the adult patients. To quote from the paper (the numbers and the word change were added for clarity by me):
“The abuse categories were: (1)recurrent physical abuse, (2)recurrent severe emotional abuse, and (3)contact sexual abuse. The five categories of household dysfunction were: growing up in a household (4)where someone was in prison; (5)where the mother was treated violently; (6)with an alcoholic or a drug user; (7)where someone was chronically depressed, mentally ill, or suicidal; and [sic. i.e., or] (8)where at least one biological parent was lost to the patient during childhood–regardless of cause. An individual exposed to none of the categories had an ACE Score of 0; an individual exposed to any four had an ACE Score of 4, etc.”
Then the researchers correlated the ACE score of each patient with the current state of health of the patient. The results are amazing. Here is one (emphasis is the author’s).
“Chronic obstructive pulmonary disease (COPD) also has a strong relationship to the ACE Score, as does the early onset of regular smoking. A person with an ACE Score of 4 is 260% more likely to have COPD than is a person with an ACE Score of 0. This relationship has the same graded, dose-response effect that is present for all the associations we found. Moreover, all the relationships presented here have a p value of .001 or stronger.
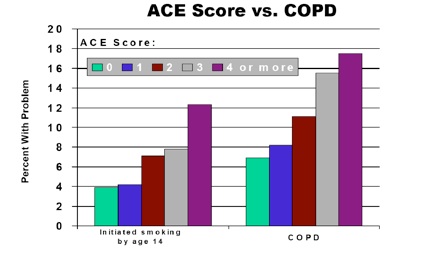
…”
Emotional disorders are also considered:
“When we looked at purely emotional outcomes like self-defined current depression or self-reported suicide attempts, we find equally powerful effects. For instance, we found that an individual with an ACE Score of 4 or more was 460% more likely to be suffering from depression than an individual with an ACE Score of 0. Should one doubt the reliability of this, we found that there was a 1,220% increase in attempted suicide between these two groups. At higher ACE Scores, the prevalence of attempted suicide increases 30-51fold (3,000-5,100%)! Our article describing this staggering effect was published in a recent issue of the Journal of the American Medical Association. Overall, using the technique of population attributable risk, we found that between two-thirds and 80% of all attempted suicides could be attributed to adverse childhood experiences.
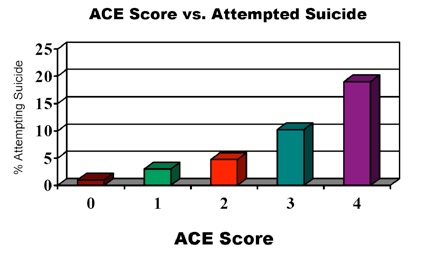
…”
There is no mention of school performance having been measured, but the following sentences appear.
“Occupational health and job performance worsened progressively as the ACE Score increased. Some of these results are yet to be published….”
Bottom line. By now you see where I am going with this. It could well be that already existing data show correlations between school performance and Adverse Childhood Experiences.
If a connection between ACE Score and school performance is known, it must be put into the public conversation about education. If it is not known, there must be research examining this possibility.
My own informal research strongly suggests a correlation between poverty and several of the categories in the ACE Score. [4]
Lesson 3. The author of the paper finds that the results of the study seriously question the investigators’ conceptual frameworks as physicians (the added emphasis is mine):
“Clearly, we have shown that adverse childhood experiences are common, destructive, and have an effect that often lasts for a lifetime. They are the most important determinant of the health and well-being of our nation. Unfortunately, these problems are painful to recognize and difficult to deal with. Most physicians would far rather deal with traditional organic disease. Certainly, it is easier to do so, but that approach also leads to troubling treatment failures and the frustration of expensive diagnostic quandaries where everything is ruled out but nothing is ruled in.
Our usual approach to many adult chronic diseases reminds one of the relationship of smoke to fire. For a person unfamiliar with fires, it would initially be tempting to treat the smoke because that is the most visible aspect of the problem. Fortunately, fire departments learned long ago to distinguish cause from effect; else, they would carry fans rather than water hoses to their work. What we have learned in the ACE Study represents the underlying fire in medical practice where we often treat symptoms rather than underlying causes.”
The author is making two points here:
1.The ubiquity and severity of the consequences of ACE make them a public health issue.
2.There is cause to question seriously the traditional medical treatment paradigm as applied to many chronic adult diseases.
Bottom line. We as educators have the same problem the doctors do. We have addressed our performance issues in terms of the variables under our control when, in many cases, the causes of what we observe in the classroom lie well outside our control. As the doctors do, we struggle mightily using the methods given to us and we get results, but often they are mysteriously disappointing. How can we expect to “teach” a child who is not present?
* * *
It is not politically correct, and we educators do not have permission, to suggest that school is part of a larger social system and that a solution to our education problems requires consideration of that larger system. Indeed, the territorial ferocity surrounding the public education debate tells me that here is yet another corollary of Conway’s Law: Our solution will be no better than our ability to reorganize ourselves to encounter the system as it truly is. [5]

Endnotes
1. http://www.traumacenter.org/
2. (Recent reference needed. “Psychological Trauma”, van der Kolk, 1987, Chapter 4 is not current enough.)
3. “The Relationship of Adverse Childhood Experiences to Adult Health: Turning gold into lead,” Vincent J. Felitti (English translation of: Felitti VJ. “Belastungen in der Kindheit und Gesundheit im Erwachsenenalter: die Verwandlung von Gold in Blei.” Z psychsom Med Psychother 2002; 48(4): 359-369). The document from which the present excepts were taken was found at http://www.partnershipforsuccess.org/uploads/200701_GoldintoLeadGermany102cGraphs.pdf
a table of supporting data is at
http://www.melconway.com/Urban_Teaching/pdf/Muni-Stats.pdf .
5. Conway’s Law is a theorem in Sociology that states a relationship between the communication structure of a design (i.e., problem-solving) organization and the structure of any design (i.e., solution) it is able to produce. See the description in Wikipedia: http://en.wikipedia.org/wiki/Conway's_Law .
© Copyright 2008 Mel Conway PhD
The Public School Issue is a
Public Health Issue
Wednesday, August 13, 2008